|
Pancreatitis
This disease could follow alcohol ingestion, use of certain types of medications or the presence of gall stones. If you suspect you have this condition, seek urgent medical advice, as the case example below demonstrates.
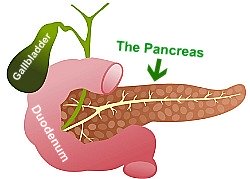
Hilary was 34. She is a top city corporate boss. She is hooked to liquor, drinking at least three to four glasses of wine every night albeit the top ups with shots of spirits at the weekends. Hilary came up with central abdominal pain that has been brewing for the past two days. The pain has become so severe that it bites deep through to the back. The pain is partially relieved by leaning forward. She vomited several times over the night. A bruising appeared on her flank, but she swore she has hot been involved in any squabble or fall. Doctors could not record her blood pressure. Within hours of hospitalization, she deteriorated so much to require admission in the intensive care unit of the hospital. By 04:00 Hours the next day, Hilary passed away, despite all the battle by nurses and doctors to save her life. So was the sad story of Hilary, an amiable vibrant young lady in Paris. Autopsy report confirmed what doctors were treating her for… acute Pancreatitis. WHAT IS PANCREATITIS? This is the medical term used to refer to the inflammation of the Pancreas. The pancreas is a comma-shaped gland lying just beneath the stomach. It plays a very important role in the digestion of food. It also helps in the regulation of the sugar level in the blood by means of two hormones it produces – Insulin and Glucagon. The digestive enzymes produced by the pancreas include lipase, elastase, protease, and amylase. The lipase help in breaking down fat and oils, the elastase, elastin, found in meat, the protease proteins, and amylase carbohydrates. These are very powerful enzymes. Even when you swallow meat in whole, these enzymes could melt the meat. The enzymes are normally channeled through special ducts as inactive chemicals into the small bowel where they act on food consumed. In this disease, their release and activation may be premature. Normally, these enzymes, apart from been released as inactive chemicals until they come in contact with the food substance they are meant to digest, their activation and actions are regulated by other chemicals produced by the pancreas. These inhibitors / regulators include C1- esterase inhibitors, alpha1-antitrypsin and pancreatic trypsin inhibitor protein. Any imbalances with this check and balance system caused by any condition precipitates an attack on the pancreas. WHY SO DEADLY? If theses enzymes come in contact with the pancreas for any reason, they promptly eat up the pancreas literally, and spread to all the surrounding tissues, causing enormous multiple tissue damage. The enzyme called lipase even convert fat found in the abdomen, lungs, knee joints and other places into soap. This occurs by breaking down fat and oil into fatty acids. These combine with calcium in a reaction called soaponification. In essence, an attack of Pancreatitis could convert a person into a “pillar of soap”! Inflammation of the pancreas is thus a very serious and potentially fatal disease. If the pancreas is damaged following an attack, the insulin producing function of the pancreas is also lost; thus, one could develop diabetes. Pancreatitis could occur suddenly and progress over days, then resolve. This is referred to as acute Pancreatitis. It could occur at a low grade level over weeks and months, referred to as chronic Pancreatitis. WHO CAN DEVELOP PANCREATITIS Pancreatitis is a relatively common illness. About 3 – 4 of every 100 person admitted into the hospital in the United kingdom for example is due to Pancreatitis. In the United States about 80,000 cases occur each year and in Japan the picture is about 21 per 100000 people. It is commoner in blacks, and can occur at any age. While generally, 1 in 100 persons having the disease could die within days, in those with severe disease, the mortality rate could be as high as 50%. CAUSES Pancreatitis can simply be caused by anything under the sun, and even the sun itself! In a less simplistic approach, causes include:
How can I know if I have Pancreatitis? (Symptoms) ACUTE PANCREATITIS Acute attack usually follows recent alcohol consumption or gallstone blocking off a duct of the pancreas. It could be caused by any of the factors mentioned above. The cause may even be impossible to identify.
Commonly, it begins with pain in the upper central abdomen, above the umbilicus (belly button). The pain could start suddenly or over quarter of an hour to a few hours, building up progressively. It is usually agonizing, and in over 50% of persons, it spread to the back. The pain may also spread to the right upper abdomen. It relieved by leaning forward in some individuals. The sufferer is usually quite sick, vomits, and may be feverish. The abdomen may be come swollen, the area round the umbilicus may become discolored to having a bluish tinge (the so called Cullen’s sign), or the flank may look bruised (Grey Turner’s sign). Patients pulse may become too fast and the blood pressure to low to be recordable. The normal sound made by the bowel may become absent. The abdomen will obviously be very tender on examination, and in severe cases, fluid would accumulate in the lung space. The patient may become confused. If the lungs, kidneys, or bowel is involved, the patient could rapidly deteriorate and death will be imminent. Sometimes, the fluid from the break down product of the pancreatic attack is enveloped by the body in what is called a pseudo-pancreatic cyst or abscess. Acute Pancreatitis could be confused with a heart attack, Cholecystitis, high bowel obstruction, peritonitis, or perforated bowel. Acute Pancreatic insult may resolve on it is own without any intervention in some cases. There is a clear responsibility on the part of the attending physician or surgeon to try and identify the precipitant of an attack of the acute disease. This is obviously to treat such where possible and prevent a second attack which could be fatal. Recurrent or progressive low grade acute Pancreatitis could lead to chronic disease. CHRONIC PANCREATITIS This results from either repeated attacks of acute Pancreatitis, or a continuing low grade unresolved acute attacks. There is a permanent irreversible damage to the structure and function of the pancreas. In prolonged cases, not only will production of digestive enzymes by the pancreas fail, there may be cessation of insulin and glucagon production once the necessary cells are damaged. This will lead to a co-existing diabetes mellitus in patients with long standing chronic disease. The ducts of the pancreas becomes distorted and narrowed due to the repeated inflammation with scar forming along it. Stones ate sometimes seen in ducts too from repeated soaponification and calcium deposits. Stones of up to 200grams have been extracted from the pancreas in chronic Pancreatic inflammation. This is the reason why prolong boring pain remains the main symptom in chronic Pancreatitis. Chronic Pancreatitis is a disease found more in middle aged men. The ratio of men to women affected by this disease stands at 4:1. It is found more after the age of 30, and peaks around the 5th to the 7th decades of live. In European countries, about 70% of cases of chronic Pancreatic irritation are caused by alcohol abuse. In Kerala, South India, most cases of chronic Pancreatitis found there are due to well established case of hereditary disease. A pointer chronic Pancreatitis is abdominal pain in anyone known to have had previous Pancreatitis, following alcohol consumption. The pain may be at the centre of the abdomen above the belly button (Epigastric region) or if the focus of the disease is mainly at the tail of the pancreas, the pain may be more towards to left (left hypochondrium). Pain may radiate to the back and or left shoulder. Pain may be relieved by leaning forward or curiously, by drinking alcohol! Nausea and vomiting may occur. There may be weight loss because of fear of eating, as eating worsens the pain. Bulky pale stool that often floats in the toilet pan is well known feature of steatorrhoea in these patients. The diagnosis of chronic Pancreatic disorder can only be confirmed with an ERCP. LAB TESTS The tests the doctors would order include: Blood Tests AMYLASE LEVELS In Pancreatitis, the amylase and lipase level is markedly increased due to this enzymes escaping into the blood from the surrounding damaged tissues. This is what doctors look out for most in blood test. Typically, the amylase level goes up to over a 200 Somogyi units. Over 1000 is almost diagnostic. Pancreatitis nevertheless is not the only condition that leads to elevated amylase level. Amylase levels are also raised in conditions like Ischaemic bowel (dying bowel due to insufficient blood supply), ruptured ovarian cyst, parotid salivary gland infection, and perforated peptic ulcer. An exceptionally high level plus a good history makes the diagnosis quite likely. Continuously elevated level of amylase suggests the formation of a pancreatic pseudocyst. Another blood test that is useful in Pancreatitis is the lactate level. CRYO – REACTIVE PROTEIN (CRP) This is a very important component of the blood test that is requested following Pancreatitis. It is also useful in determining the outcome of the disease in individuals in terms of their survival. C-reactive protein is a protein produced in response to ANY acute inflammatory process in the body. It would thus be elevated in Pancreatitis. It starts to subside once the inflammatory process is resolving. If the level continues to be high in the first 96 hours after show a significant disease. FULL BLOOD COUNT (FBC or CBC) Full blood count may reveal a raised level of white blood cells. This raised levels could be strictly from the inflammatory process going on or commonly, from bugs (bacteria) breeding in the soup of dead tissues produced following inflammation of the pancreas. The white blood cells would go from upward of 12,000. The creatinine and urea levels may also be elevated. An arterial blood gas level may also be requested. There may be a reduction in the pH (acidosis) if compensation has not taken place plus a base deficit.In severe cases, oxygen level would be low. Urine Test After two to three days of the onset of acute Pancreatitis, the blood amylase level could start to reduce. A sure way of telling if the suspicion of Pancreatitis was right is to do the urine amylase: creatinine level. It is usually raised. X-ray A plain abdominal X-ray may show little or nothing. Must often, a small loop of dilated small bowel can be seen in acute Pancreatitis X-ray referred to as the sentinel loop. Of more importance is an erect chest X-ray. This helps to demonstrate air under the diaphragm if the symptom been investigated is due to a perforated bowel which could present virtually like Pancreatitis. If the lungs are involved in Pancreatitis, the chest x-ray may show signs of fluid collection in the lungs or its coverings. Ultrasound Scan Ultrasound scan is the gold stand for confirmation of the diagnosis of Pancreatitis. It will demonstrate a swollen pancreas, and free fluid in the abdomen. It could also tell if the cause of the Pancreatitis is due to gall bladder stones as this will show up in the ultrasound scan. CT – Scan In acute disease, CT scan done after a couple of days will shed light on the viability of the organ, and how much of it is left. This will also demonstrate the involvement of adjacent organs and the bowel. This is the most useful mode of investigation in chronic Pancreatitis. Its sensitivity is 75 – 90 % in chronic Pancreatic inflammation, and detects calcification, obstruction along the ducts, and any abnormality of the sounding organs like the spleen. Endoscopic Retrograde Cholangio-Pancreatography (ERCP) TREATMENT OF ACUTE PANCREATITIS The acute disease is an emergency. Once it is suspected from the history, the doctor will order the various test and start treatment immediately.This includes: Pain control Giving fluids through the veins to replace fluid lost Oxygen Antibiotics Putting in urine catheter to collect and most importantly monitor the function of the kidney Ask that nothing else be eaten Introduce a naso-gastric tube Very ill patients are best transferred to the high dependence unit of the hospital for close management. If there is high blood glucose level, the patient is given insulin. Giving injection to thin the blood as well as wearing an anti leg blood clot stockings is highly recommended. Look for possible reversible precipitants like medications. TREATMENT OF CHRONIC PANCREATITIS Pain management Pain management is the main stay in chronic Pancreatitis. A wide range of pain killers are available for use including NSAIDS like ibuprofen and volterol. DIET The diet should be one very low in fat. Alcohol should be totally avoided in these patients. Pancreatic enzyme supplements are available. This helps restore the lost digestive function of the pancreas to a reasonable level. The use of morphine and tobacco is also to be discouraged.
|
[?]Subscribe To This Site
|



